What to do with oral formulations that cannot be cut or crushed?
Authorr: Dr Peter Dvorak. Pharm.D.,DESS.,CTH.
There are several situations where changing an oral formulation may be useful or even necessary. However, these manipulations can sometimes have disastrous effects on the health of patients. Currently, to our knowledge, there is no guide in Canada as to which oral drug can or cannot be modified. American and European publications, on the other hand, are difficult to adapt here, because the names and formulations are different. In this article, we will discuss the different oral formulations as well as the reasons why we can or cannot change them.
From the moment it is prescribed until the moment it is administered, the oral medication goes through several voluntary manipulations that can modify its physical integrity. Whether by pharmacy staff, the one administering it to the patient, the caregiver or the patient himself, the medication can be divided, crushed, dissolved, mixed with food or chewed. A problem may arise when these manipulations of the oral formulation influence its pharmacokinetics to the point of altering its therapeutic efficacy. There may then be a decrease in the effectiveness of the product, underdose, overdose or adverse effects. Unfortunately, these situations are happening more and more often, as an increasing number of drugs cannot be changed1,2.Some products are derived from high-tech processes, with specific physicochemical properties. That is why dividing or grinding them destroys the intended mode of release and can have serious consequences. Unfortunately, it is reported in the scientific literature that in many long-term care facilities, drugs are routinely crushed without reference to relevant sources.3-7. Deaths or serious adverse events have occurred in hospitals where caregivers had crushed Adalat XL® and Oxycontin® tablets. Recently, hundreds of deaths have occurred in the United States in people who illegally abused oxycodone by crushing long-acting tablets8 . In a 2005 pilot study by a UK pharmacy with elderly patients, 58% of people reported opening capsules or crushing tablets to make them easier to take, and 65% believed that crushing the tablet or opening the capsule did not affect the effectiveness of the drug9,10.It is obvious that if one refused from the outset to cut or crush all the tablets, one would then deprive many patients of the benefits of these drugs. Some may even be deprived of treatment. The solution is to increase knowledge of the characteristics of solid oral formulations and why they can or cannot be modified. The various stakeholders will then be able to make an informed decision on the subject or choose a valid alternative. They will also be able to effectively inform their patients and the providers who help them.
This article is intended to be a practical and theoretical overview of the different oral pharmaceutical formulations, their properties and the constraints associated with each of them. Some information relates to practical experience and information obtained from pharmaceutical companies, as the scientific literature offers little information on the possibilities of modifying oral pharmaceutical formulations.
In addition, pharmaceutical companies’ information centres should not be underestimated. They hold impressive data on their products and one should not hesitate to consult them when needed.
Why change oral formulations?
Change the dose.
Over the past 20 years, the amount of drugs available on the market has increased exponentially and therapies have become increasingly complex. We try to individualize treatments, to favor combinations of drugs with low doses to reduce the incidence of adverse effects. For example, in the treatment of arterial hypertension, we are faced with situations where certain low doses are not on the market, for example metoprolol 12.5 mg, hydrochlorothiazide (HCTZ) 6.25 mg or bisoprolol 2.5 mg, doses that are recommended clinically. We are treating an increasingly aging population that suffers from hepatic and renal failure or low weight. In addition, several drugs not available in liquid formulations will be used in the pediatric population. Can we cut these tablets without question?
Even if the tablet is scored, a whole tablet should always be preferred. Halving a tablet may result in uneven distribution of the dose in both halves of the tablet.11 The active ingredients can also degrade in contact with air, moisture or light. For this reason, whenever possible, tablets should not be cut several days in advance.11,12. If the tablet is to be divided, the size, shape and fragility of the tablet will need to be considered, as these factors affect the accuracy of sharing. Elongated tablets with deep grooves on both sides are the easiest to cut11. The risk is probably minimal when cutting drugs with a long half-life and a broad therapeutic index such as those used for hypertension and dyslipidemia.13. On the other hand, extreme caution should be exercised when deciding to divide tablets containing active ingredients with a narrow therapeutic index (digoxin, lithium, theophylline, warfarin) or a liquid formulation should be preferred.11. Caution should also be exercised when dividing tablets, which are combinations of products, unless grooved. Indeed, it is difficult to be sure of the homogeneity of the mixture of active ingredients in the tablet13. The sharing of tablets should be carried out at the pharmacy, using a tablet cutter, by a person authorized to do these manipulations and not by the patient himself11,12. Unfortunately, we still too often see patients who leave the pharmacy with unsevered tablets without instructions and divide them at home in a rudimentary and imprecise way. Indeed, a recent review of scientific literature found very significant dose differences when sharing tablets, up to plus or minus 50% of acceptable weight.13.
Swallowing difficulties
Dysphagia is a very common problem in the general population. In the United States, more than 18 million adults suffer from it14. This number will tend to increase because of the aging of the population. A recent U.S. survey found that 40% of adults reported having difficulty swallowing their tablets. Of these patients, 14% delayed taking their dose and 8% missed taking it14. Among patients in long-term care facilities, between 30% and 60% of residents suffer from dysphagia to varying degrees. Several factors can contribute to causing dysphagia. Up to 40% of stroke patients and 50% of Alzheimer’s patients will have swallowing problems9,15,16. Cancer or related treatments, tumors of the oropharyngeal region, Parkinson’s disease, xerostomia, nerve damage in the oropharyngeal region are other causes contributing to dysphagia17. Certain medications such as neuroleptics, tricyclic antidepressants, antihistamines and anticholinergics can also aggravate this problem.17.
When abnormally large tablets are to be dispensed, the patient’s experience with large tablets should be checked with the patient at the outset. If the doctor says he will have difficulty swallowing them, check before cutting them to see if he can give him the same dose with tablets of lower strength, usually smaller. As an example, we can mention the Cipro XL® 1000 mg, a huge tablet that can be substituted by two smaller tablets of Cipro XL 500 mg. This is the case for several antibiotics such as Keflex® 500 mg, Ceftin® 500 mg, Cefzil® 500 mg, Biaxin® 500 mg, Levaquin® 500 mg, but also anticonvulsants such as Tegretol CR® 400 mg (available in 200 mg).
In the case of more severe dysphagia, when the tablet can be crushed, it is necessary to ensure that the operation is done with appropriate tools, namely a pestle and a mortar and that the entire dose is given (watch out for the powder that remains stuck on the pestle and the sides of the mortar)3 . The crushed tablet should be incorporated into a small amount of a semi-solid or liquid food depending on the physicochemical properties of the drug and administered immediately. When administering several tablets, each drug should be given separately to avoid incompatibilities. The majority of tablets made of compressed and uncoated powder are designed to disintegrate quickly in the stomach and therefore can be crushed beforehand.18,19. Some medications can also be dissolved in water, which is then drunk by the patient. This is the case of Nexium. Others are available in chewable form such as Tegretol chewable tablets. There are also a variety of medications in orodispersible tablet form such as Zyprexa Zydis®, Prevacid FasTab®, Maxalt RPD® and others. Placed on the tongue, these tablets disintegrate very quickly and can be swallowed without difficulty. The active substance remains in microgranules that are absorbed into the gastrointestinal tract. A recent study seems to show efficacy and preference of this formulation in patients with dysphagia14. Some products are also available in sublingual form and can be used in this way, such as Ativan® S/L. As for hard gelatin capsules (capsules), which we will discuss in detail later, it should be noted that most can be opened and the contents mixed in the same way as a crushed tablet. If the capsule contains coated microgranules (Cardizem CD®, Sporanox®, Prevacid®, etc.), these should not be chewed. In some cases, liquid formulations can replace tablets, but doses are not always equivalent. If applicable, dose equivalence for a given product should be required, dosage adjustment if necessary, and clinical follow-up should be performed as needed (e.g., Dilantin® capsules versus oral suspension formulation).
The use of non-oral formulations for this type of patient should not be neglected. Many medications are available in the form of skin patches such as hormone replacement therapy (Estraderm®, Estradot®, Estalis®, Androderm®), nitrates (Nitro-Dur®, Minitran®), opioid analgesics such as fentanyl (Duragésic®), oxybutinin (Oxytrol®) or oral contraceptives (Evra®). Others are available as skin gels such as hormones (Estrogel®, Androgel®) or anti-inflammatories (Pennsaid®). Rectal suppositories are a very relevant option, because they are easy to administer and they cover several therapeutic classes, including analgesia (acetaminophen, ketoprofen, naproxen, indomethacin oxycodone, etc.). Rectal oral administration is not recommended as there are limited pharmacokinetic data for this use. Kinship routes such as the subcutaneous route are impractical in ambulatory patients and are mainly used in the context of palliative care.
In closing, when a tablet cannot be crushed and the drug does not exist in another formulation, it can always be replaced, after intervention with the prescriber, with a drug of the same therapeutic class that can be modified. For example, in the class of calcium channel blockers, an osmotic nifedipine system such as Adalat XL could be replaced by a breakable amlodipine tablet (Norvasc MD).
Cost reduction
In 2003, U.S. Veterans Affairs saved about $46 million by routinely offering half tablets of simvastatin 40 mg instead of one 20 mg tablet. It would seem that the effectiveness of the treatment was not affected by this substitution20. We see this trend in some prescribers who suggest that patients split the Proscar® (finasteride 5 mg) tablets indicated for benign prostatic hyperplasia into four pills, in order to obtain an equivalent of Propecia® (finasteride 1 mg) indicated for the treatment of alopecia, which is more expensive and not covered by insurance. Others prescribe half tablets of Lipitor® (atorvastatin) 20 mg or 40 mg to save the patient. Unless there are exceptional cases, these trends should be discouraged, especially given the lack of clarity on tablet sharing. In addition, the American Pharmacists Association and the American Medical Society oppose the systematic division of tablets.13. Instead, the solution to the cost of the drug is generic substitution of bioequivalent drugs or the prescription of less expensive therapeutic equivalents.
Potentially non-modifiable oral formulations
Coated tablets
Tablets with gastrosoluble coating
Some coated tablets are covered with a film or layer sometimes smooth and transparent, more often shiny and curved, of bright and varied color, also called film-coated tablets. This coating is gastrosoluble and is used to facilitate swallowing, improve its presentation and allow the identification of the drug. It can also mask the taste and protect the active ingredient from light and moisture.18,21. The cross-section of these tablets is difficult, because because of the curved shape and coating, the halves are often inaccurate. On the other hand, with the exception of active ingredients irritating to mucous membranes, tablets can be ground into powder, if the patient accepts the taste18,21. Obviously, the drug must be administered quickly, especially if the active ingredient is sensitive to moisture or light. The situation is quite different with gastro-resistant or enteric-coated tablets, which cannot be modified.
Enteric-coated tablets
The gastroresistant coating prevents the dissolution of these tablets in the acidic environment of the stomach. There are several reasons for using this pharmaceutical form. Inactivation of the active substance may be prevented, irritation of the gastric mucosa may be prevented or the onset of action may be delayed.18,21,22. It is also possible to target the area in the gastrointestinal tract where the drug is to dissolve and be absorbed, using a pH-dependent dissolution coating. It is easy to understand that the destruction of this coating by cutting or grinding will result in a decrease or suppression of effectiveness or the appearance of adverse effects. However, there is an exception: some of these pharmaceutical forms can be powdered and then administered through a duodenal or jejunal tube.12,21. Caution is still advised since the acidic duodenal pH can be harmful for some active ingredients.
Active substance inactivated by gastric juice
Several medications must be protected from gastric acidity by a coating that prevents the dissolution of the tablet in the stomach. Proton pump inhibitors (omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole), used in the treatment of peptic ulcers and gastroesophageal reflux, are all acid-inactivated6,12. There was one reported case of omeprazole ineffectiveness after one month of treatment because the tablet was crushed and administered into the enteral feeding tube (gastric tube)6 . Fortunately, there are formulations in this class that can be easily modified for patients with swallowing difficulties. Prevacid is a capsule with gastro-resistant granules that can be opened and sprinkled extemporaneously on applesauce23. It is important to mention not to chew the granules. The same medication is also available as an orodispersible tablet (Prevacid Fastab). Nexium is an ANTRAMUPS® tablet, which contains gastro-resistant microbeads. It can be dispersed in two to three minutes in 20 mL of water or orange juice, then administered quickly, being careful not to chew the microbeads.21,23.
Pancreatic enzyme supplements (amylase, lipase, protease) are another type of active ingredient that can be inactivated by gastric juice. Again, there are several formulations in capsule form with gastroresistant granules (Cotazym ECS®, Creon®, Pancrease MT®, Ultrase MTMD, etc.).23 which can be opened and sprinkled as described above. However, prolonged contact of the granules with the oral mucosa or hands should be avoided because of the irritating potential of the enzymes21,23.
Active ingredient too irritating

There are active ingredients that can damage the gastric wall, either in patients with already existing sensitivity (irritation, history of ulcerative disease, risk factors, elderly patients, etc.), or because high doses or prolonged treatments are given. This is the case of nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, ferrous sulfate, potassium, etc.24 (Naprosyn EMD, Entrophen®, Slow-KMD). The gastrorestic coating protects the stomach lining from direct contact with the irritant substance and, therefore, it must not be altered. There are alternatives in the form of chewable tablets (Motrin®, Advil®, Aspirin® 80 mg chewable tablets), suspensions (Naprosyn® oral suspension 25 mg/mL, Palafer® suspension) or uncoated tablets that can be cut or crushed.23. As for NSAIDs, their pharmacological effect on prostaglandins greatly contributes to the adverse effect on the gastric mucosa, in addition to the local effect of the active ingredient. Therefore, cytoprotection should be provided in patients at risk, regardless of whether the formulation is enteric-coated or not. Another valid solution is to use substances of the same therapeutic class with less irritant properties and can be modified. Mention may be made, in the class of NSAIDs, COX2 inhibitors such as Celebrex® and Mobicox® 23.
Active substance to be released at a specific location 5-amino-salicylic acid (5-ASA)
Preparations containing 5-ASA are used to control the symptoms of inflammatory bowel diseases such as ulcerative colitis and Crohn’s disease. In order to target the action of the drug to specific locations in the gastrointestinal tract, some formulations have a pH-dependent acrylic coating. Asacol®, Salofalk® and Mesasal® release their active ingredient into the terminal ileum and colon where the pH is greater than 723. Therefore, an alteration of this coating would significantly alter the expected effect of the drug and the effectiveness of the treatment.23.
Extended-release oral formulations
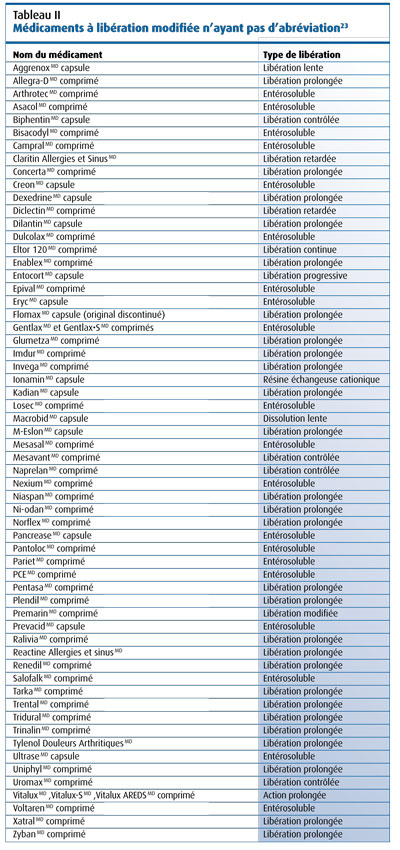
These formulations consist of a high dose of active ingredient that will be released gradually and sustainably over a long period of time. This ensures a stable therapeutic blood level for an extended period of time, thus reducing the number of daily doses and promoting adherence to treatment. In addition, adverse effects are also reduced by attenuating the blood peak compared to the same dose that would be administered in an unmodified dosage form.25-27. Thus, long-acting nifedipine (Adalat XL) prevents sudden hypotension and reflex tachycardia following administration26. There is also a decrease in sleepiness with carbamazepine CR and a reduction in nausea with prolonged formulations of theophylline.26. These advantages have contributed to a strong growth of these products in the market. In 2001, these formulations already accounted for 15% of the total market for medicines.27.These drugs are fairly easily recognized by the abbreviations that follow the name such as XL, CD, CR, LA, SR, SA, PA, XR, contin (continuous action) and 12H or 24H. These abbreviations are explained in Table I. 23,28. Several interchangeable terms are also used to describe these formulations. We can talk about sustained, extended, controlled, progressive, slow release (slow-release, long-action), etc. On the other hand, we must remain very vigilant, because some names that do not contain abbreviations are still extended-release formulations (Table II).23. Now let’s see the different formulations on the market.
Osmotic pumps

These are actually small tanks where the active ingredient is contained in an indigestible core and covered with a semi-permeable membrane. The tablet has a small laser-pierced opening. In the gastrointestinal tract, water passes through the membrane by osmosis, disperses the drug and expels it through the opening at a constant rate. There are several variations of this system including push-pull®, l-oros® and OROS Tri Layer® osmotic pumps. In the push-pull system, the tablet consists of two compartments, only one of which contains the active ingredient. Water enters the inactive compartment by osmosis (osmotic motor). A polymer swells and exerts pressure on the compartment containing the drug. The latter will therefore be expelled through the opening in the tablet and this at a constant speed (Figure 1). The L-OROS system is a soft gelatin capsule and the OROS Tri Layer consists of three compartments, two of which contain the active ingredient. An alteration of the membrane of one of its systems, by section or grinding, would cause an immediate release of the drug and a risk of overdose23. Osmotic pumps are used in several drug formulations including Adalat XL, Ditropan XL®, Concerta, etc. Photos of several formulations can be seen in Figure 2.

Matrix systems
These are most often insoluble porous materials in which the active ingredient is dispersed. The material consists of physiologically tolerated products such as waxes (carnauba wax) or polymeric substances25,26. The active ingredient is trapped in this porous network. It diffuses gradually as water from the gastrointestinal system seeps into the matrix according to predetermined physicochemical characteristics. The section of the tablet is theoretically possible, because the surface of contact with the surrounding environment is not significantly increased. On the other hand, grinding these tablets is contraindicated, because it substantially increases the contact surface as well as the rate of dissolution and absorption of the active product. Examples of these products include Mestinon® SR, Duralith®, Imdur®, Phyllocontin®, etc.23,25,26.
Some matrices are also partially soluble. In these cases, the release of the product is controlled by the erosion rate of the matrix. An example of this formulation is Sinemet CRMD 26.
Other formulations

Other modified-release formulations exist on the market. Multilayer tablets (Xatral®, Claritin Extra®, Allerga DMD) can be used to separate incompatible active ingredients or to use different dissolution rates from one layer to another (Figure 3). This last formulation makes it possible to have a loading dose and a maintenance dose for the same active ingredient or an immediate effect dose of the first drug, then a prolonged effect of the second active ingredient21,23.
Other techniques are also used such as different dissolution rates between complexed or free molecules, between polymorphic crystalline forms or ion exchange resins.26.
Some of these formulations can be sectioned, others cannot. We use case by case to determine what can and cannot be done with these formulations.
Sublingual and orodispersible formulations
Although these two types of formulations are sometimes confused, there are fundamental differences between them. Sublingual tablets are designed to be absorbed through the oral mucosa. They must be kept under the tongue where they will be absorbed thanks to the large blood flow to this area24,28. For some formulations, being crushed and swallowed can decrease their effectiveness which is based on sublingual absorption24,29. They also have a faster onset of action than traditional formulations, because the active ingredient enters directly into the bloodstream. This type of tablet can be an interesting option for a patient with swallowing problems as long as he is able to hold the tablet long enough under the tongue and does not suffer from severe xerostomia. However, there is not a large selection of these products. Examples include Ativan S/L, Nitrostat®, etc.
Orodispersible tablets are designed to make it easier to take during swallowing difficulties. They must be placed on the tongue and are dissolved quickly by saliva in order to be swallowed more easily14,21. It should be noted that their action is not faster than that of the corresponding traditional forms21. Indeed, they are composed of microgranules that reproduce as much as possible the release of a conventional tablet. More and more drugs are available in this formulation because it meets a need, especially in the geriatric population.

Sublingual and orodispersible formulations are generally very friable. Therefore, it is not recommended to cut these types of tablets23.
Capsules and capsules with coated microgranules
Soft gelatin capsules or capsules are composed of a single airtight piece of gelatin and contain the drug in liquid form often lipophilic (Figure 4). In the stomach, the envelope dissolves quickly, usually in three to eight minutes, and releases the active ingredient. Although it has already been recommended to dissolve the capsules in a little warm water, the oily content often makes this preparation difficult for the patient to accept.21. Piercing the capsule and recovering its contents is generally not recommended. The operation is too imprecise, because the exact dose cannot be recovered. Finally, the capsules are also used to protect the oral and pharyngeal mucosa from the irritative effect of certain substances such as isotretinoin (Accutane®, Clarus®) and valproate (Depakene®)23. Many products are found in the form of hard gelatin capsules that contain microgranules, either with a gastroresistant coating (enzyme complexes), or coatings of different thicknesses, therefore with different dissolution rates (Cardizem CD®, Adderall XRM®, Tiazac®, etc.) or a mixture of immediate-release and extended-release active ingredients (Aggrenox®) (Figure 5). Most of these capsules can be opened and their contents mixed with a little semisolid food (compote, pudding, etc.) and swallowed without chewing the microbeads23.
Formulations that are dangerous for personnel handling them

Two types of formulations fall into this category. First, nitroglycerin-based drugs (nitroglycerin, mononitrate and isosorbide dinitrate) have a theoretical risk of explosion if crushed or sprayed31. Although no cases have been reported, it is contraindicated to crush this type of tablets. Second, all cytostatic or antineoplastic drugs can be dangerous to the personnel who crush them. Indeed, the spray of these tablets projects powder into the air which is then inhaled by the personnel28,31,32. The American Association of Hospital Pharmacists proposes a simple method to safely crush antineoplastics7 . The tablet is placed in a small sealed plastic bag (Zip-Lock type), then crushed with the pestle carefully so as not to pierce the wall of the bag7 . The crushed contents can then be incorporated into semi-solid food following the usual precautions such as wearing gloves. This method can be used to crush any type of tablet, as it helps prevent a loss of medication that remains stuck on the pestle or in the bottom of the mortar.
Conclusion
Over the past several years, there has been a significant increase in the number of modified-release drugs in the Canadian market. As a result, more and more oral medications cannot be modified to facilitate administration. Changing these formulations can have serious consequences for patients’ health. The pharmacist is often consulted on this subject and must have up-to-date tools and knowledge in order to effectively answer these questions. It is also an opportunity for him to assert his expertise as a drug specialist. A list of oral formulations that cannot be modified, updated regularly, as well as an increased knowledge of the oral formulations available are essential tools in these situations.




